Rutgers Arm Virtual Rehabilitation for Patients Post-Stoke and Post-Severe Traumatic Brain Injury
Project Overview
- What's the problem?
- Why Virtual Rehabilitation?
- What we've done?
- Who was included?
- The exercises/games.
- What have we found?
- Related publications.
- Supported by:
- Press Releases.
- Project Video - Participant feedback following Rutgers Arm Feasibility Study. (~35mb MPEG4)

-
What's the problem?
-
Why Virtual Rehabilitation?
-
What we've done?
-
Who was included?
-
The game exercises.
-
The Baseline Exercise
-
The Pick-and-Place game
-
Breakout 3D game
-
Treasure Hunt game
-
Card-Island game
-
Tower Of Hanoi 3D game
-
What have we found?
All the participants showed improvement in their skills after the study. The stoke survivors showed improvement in their affected upper extremity when compared to their initial level of function. They were able to complete daily tasks such as picking up a glass, tying shoe-laces, buttoning clothes, and opening doors more easily when compared to pre-study testing. Grasping strength increased as did active range of motion. A stroke survivor, who was not able to open a car door, feed himself or shovel snow using his plegic arm, could do so after training.

Participant opening a car door post-training.
Participant feeding himself post-training.
Participant shoveling snow post-training.The TBI patients also shows showed improvement in upper extremities when compared to their initial level of activity. They also showed improvements in cognitive skills such as memory and free-recall of visual information. All participants showed more confidence in completing daily activities when compared to pre-study testing.
All the participants did not show much of an improvement in verbal skills as most of the games dealt with visual and motor training.
Each year about 1.7 milion Americans suffer from Traumatic Brain Injury (TBI) and another 800,000 Americans suffer from a Stroke. TBI causes can range from accidents (motor-vehicle, sports, military) to abuse. These patients present diminished executive functions, difficulty focusing, and degraded short term memory.
Stroke is a cerebrovascular accident caused by hemorrhage or blockage of the blood vessels in the brain. This results in paralysis of the contra-lateral half of the body.
These patients require upper extremity motor relearning, as well as strengthening of their affected shoulder and hand.
Virtual reality offers a number of advantages compared to conventional therapy, including the ability to gradate game difficulty and adapt each game to a given patient in a given day. Therapy in the form of games mediates the needed number of repetitions so to induce brain plasticity. Yet games (if winnable) keep the patient engaged and focused, as opposed to being bored by too many repetitions. Finally, virtual rehabilitation is known to provide substantial knowledge of results, which is a key factor in rehabilitation.
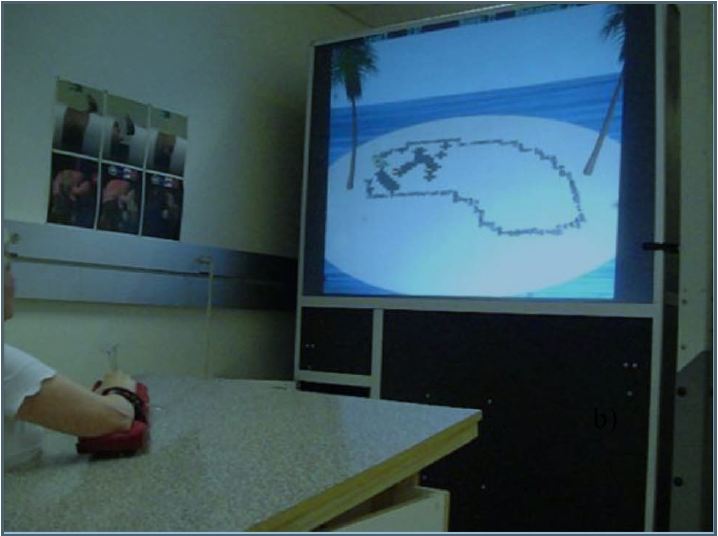
A light-weight sensorized forearm support was built. The forearm support has embedded sensors to detect the patient's arm movement and a deformable rubber pear connected to an air pressure sensor that detects grasp strength. All these sensors transmit information wirelessly to a computer that records all the data.
A low friction, tilting table was also built. The table can tilt up 0°, 10°, 15°, 20°, 25°, or 30° by placing pairs of spacers under the top surface frame. Tilting is intended as a way to apply modulated load on the trained arm. Tilting the table upwards makes arm movement away from the trunk more difficult, while tilting the table downwards assists these movements. Forearm weights can be attached to the patient's arm for addition gravitational load.
Using this forearm support, the patient places his affected arm on the table and plays 5 different games that help retrain motor and cognitive skills. The movement on the table is mapped to avatar objects displayed on a large projection-based display faced by the patients.
The study received approval from Institutional Review Board at Rutgers University. Patients who were either stoke survivors or had sustained a severe TBI were selected.
Seven patients, aged 46-70, who had suffered a stroke were selected for the study. Each participant had a stoke of varying severity 12-42 months before the trail, which affected their right upper extremity (arm, shoulder, hand). They had undergone traditional physical or occupational therapy that lasted 1-6 months. At the start of our experimental therapy, two patients presented with high spasticity which prevented them from using their plegic arm in activities of daily living. The patients suffered from mild to medium loss of hearing, vision, and touch. All the patients were taking medication to keep their blood pressure and cholesterol in check. A few patients were also taking anti-depressants.
Two partcipants, aged 23-33, had suffered a severe TBI due to motor vehicle injuries. They had undergone extensive PT/OT to regain basic motor skills after their accidents, however one patient had difficulty using her left arm, had abnormal hand/wrist posture and substantial weakness in her upper extremity. Both participants had had psychological counseling. However, their cognitive functions were still impaired in the areas of attention, memory, executive functions, visual-spatial ability, verbal fluency, and basic auditory and visual attention.
All participants received medical clearance from their physician and signed a Consent/Assent Form approved by the Rutgers Institutional Review Board (IRB). Training took place at the Rutgers Tele-Rehabilitation Institute, Piscataway, NJ.
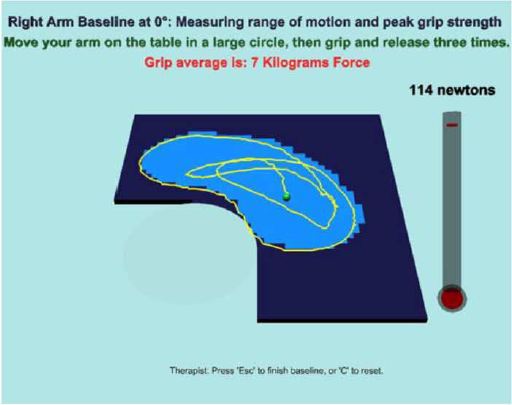
The Baseline exercise is aimed at measuring the affected arm's table-supported range of motion and hand grasping strength. The area that the client can reach with the affected arm, while sitting comfortably without leaning, represents the reach baseline. It is measured at the start of each session and is client-, date-, and table tilt-specific. The client is instructed to "clean" the table avatar as much as possible, by moving the affected arm without leaning. The area the client is reaching is interactively updated, while the tracking software monitors trunk leaning. Depending on the leaning threshold, the arm reach baseline exercise records an approximation of the client's actual capability that day. The grasp strength baseline exercise immediately follows the arm reach baseline. The client squeezes the rubber pear in the arm support, while a thermometer-like gage to the side of the screen shows the peak grasp force. The system averages three maximum voluntary grasps, and the value is displayed at the top of the screen. A percentage of this average (set by the therapist at 25% in this study) is subsequently used as a threshold to detect momentary grasping during games. This percentage is in line with studies on post-stroke grasp strength and fatigue as a percentage of Maximum Voluntary Contraction.
The Pick-and-Place game trains motor control and grasps strength in the upper extremity. The client is asked to closely follow a prescribed path. The location of the ball and target is a function of the arm reach baseline, assuring that the client is capable of executing the extent of the movement. The client first overlaps a hand avatar over the ball and squeezes above a threshold to pick the ball up. Subsequently the client can relax the grasp and place the ball into a rectangular target area, while following a prescribed path. Depending on the relative positions of the ball and the target, the trained movement requires alternating sequences, abduction/adduction, flexion/extension, or combination of both. When the table is tilted up, movement away from the body is resisted by gravity, and that towards the body is assisted. The game displays a trace of the actual hand movement, overlaid on the prescribed (ideal) path. This knowledge of result allows the participant to judge immediately how close the prescribed path is followed. At the end of a number of pick-and-place repetitions, summative knowledge of result is provided in the form of a bundle of traces. The more uniform the arm movement and the closer to the prescribed path, the tighter this trace bundle is, and the less wavy it is. This graphical knowledge of result is supplemented numerically by the path error representing the closeness between the actual path and the prescribed one, over a number of trials. The design of this game is in line with motor learning theory which emphasizes practice through repeated execution of a movement, and transfer to function. The transfer to function relates to pick-and-place activities where hand motion generally follows a straight trajectory.
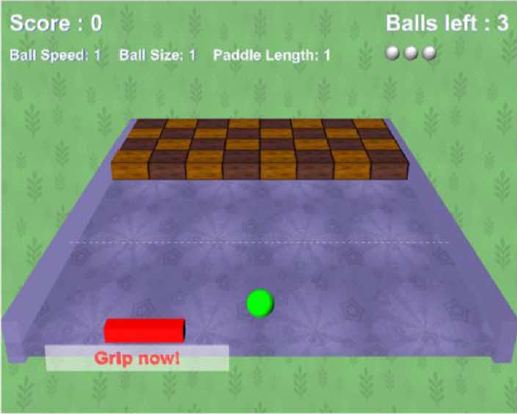
The Breakout 3D game was developed to train hand-eye coordination, arm speed of movement, and dual-tasking. The client is tasked with destroying an array of cubes by bouncing a ball off a paddle avatar controlled by the affected arm. Depending on the orientation of the cube array, the game induces mainly flexion/extension (in-out) or abduction/adduction (left-right) arm movements. The extent of arm reach in either direction, measured at baseline, is mapped to the paddle excursion on the playing board, so that the client is able to reach any location on the board. The difficulty of the game is increased by making the balls faster and the paddle smaller. Additionally, participants are required to grasp above their baseline-dependent threshold just before the ball hits the paddle, otherwise the ball passes though the paddle and is lost. After each bounce off the paddle, the ball can destroy at most one cube. This feature is intended to maximize the movement needed to destroy the whole array. Knowledge of result is implicit in the ability to dynamically bounce the ball, as well as seeing the number of cubes diminish throughout the game. If the client does not move sufficiently fast, does not grasp in time, or has diminished hand-eye coordination, then the number of allowed balls is expanded early, and the cube array is only partially destroyed. Additional knowledge of result is provided as a percentage of cubes destroyed, and applause is heard once all cubes are destroyed.

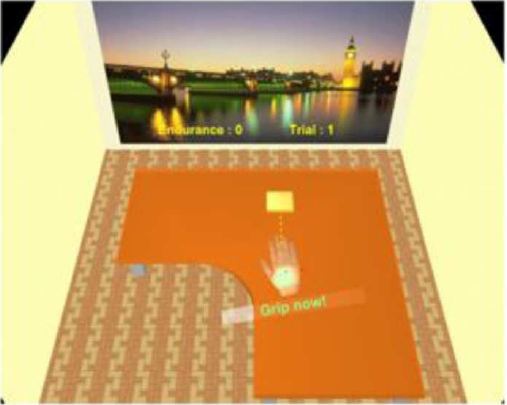
The Treasure Hunt game is aimed at increasing arm endurance, speed, and grasp strength. The game depicts an island on which a number of treasures are buried in the sand. The participant controls a shovel avatar by grasping above a threshold and digging out as many treasures as possible in the allowed amount of time. The session baseline is used to map an area on the island where treasures are hidden, which is delineated by a wall of boulders. Treasures buried closer to the boulders are worth more points if discovered, as they require movement at the extreme of arm reach. If leaning is detected, treasures remain hidden, even if the shovel avatar overlaps them. The difficulty of the game is further increased by periodic sand storms which partially cover the already-discovered treasure chests, in turn requiring more arm movement. Thus the client is motivated to move quickly, before the onset of the next storm. The more treasures are uncovered, the more points the participant scores. Knowledge of result is provided through graphics and sound by the appearance of uncovered treasures and numerically through the total gold coins found, and the number of chests remaining to be found. Additional knowledge of result is the percentage of treasures found displayed once the allowed time had lapsed. To further motivate the client, the game has the relaxing sound of waves washing on the beach, and plays applause when the client has high scores.

The Card Island game is aimed at training short term visual memory as well as grasp coordination and shoulder strengthening. The game scene is a tropical island showing an array of playing cards arranged face down on the sand. The cards are positioned inside the area that corresponds to the arm reach baseline, such that the participant can turn cards face up by overlapping them with the hand avatar. In order to turn a virtual card face up and reveal its image the participant has to momentarily grasp on the forearm support deformable element. The cards can be customized for each participant with images of pets, relatives, or other scenes of interest, so as to increase motivation. If two subsequent selections show the same image, the matched cards disappear from the island, otherwise they turn face down again. Game difficulty is increased by adding more cards, which requires more motor and grasp repetitions and increased cognitive effort for matching.
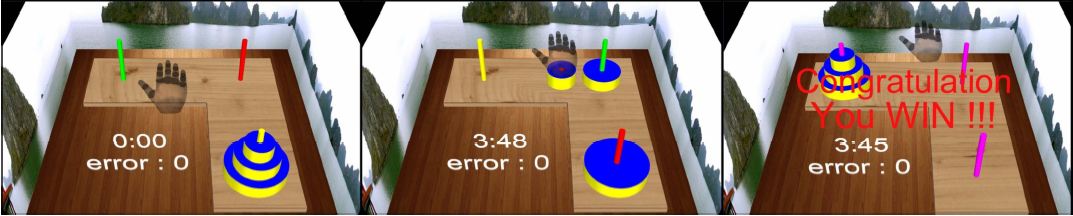
Tower of Hanoi is a classic logic and executive function game that asks players to stack disks of different diameters on one of the 3 poles. The disks are initially on one pole, stacked in increasing size from top to bottom and the player has to restack the disks on another pole in the same order of sizes, while using the third pole as a way point. During the game the disks are selected and moved with a mouse on 2D screen, and acceptable moves are dictated by the condition that a smaller disk is never to be placed under a larger one. Tower of Hanoi 3D is our version of the well-known game just described. It presents a 3-D scene showing 3-D disks, 3-D poles and a hand avatar controlled by the participant's arm movement and grasping. The poles are placed inside the participant's arm reach area, and participants had to overlap a disk with the hand avatar, and then grasp to pick it up and subsequently place it precisely on a desired pole. The continuous grasp condition was set when training dual-tasking. In such setting the participant had to maintain gasp strength above a threshold, else the disk fell en route and had to be picked up again. Game difficulty was increased by adding more disks, which corresponded with a larger sequence of moves needed to restack the disks. Thus Tower of Hanoi 3D trained not only logic and executive function but also motor control, shoulder/grasp strengthening and dual-tasking.
-
Related publications.
-
G. Burdea, D. Cioi, J. Martin, B. Rabin, A. Kale, and P. DiSanto, Motor Retraining in Virtual Reality: A Feasibility Study for Upper-Extremity Rehabilitation in Individuals With Chronic Stroke, Journal of Physical Therapy Education 25, 1:20-29, Winter 2011. Full Text PDF
-
G. Burdea, B. Rabin, A. Chaperon, J. Hundal, Emotive, Cognitive and Motor Rehabilitation Post Severe Traumatic Brain Injury - A New Convergent Approach, Proceedings of the International Conference on Virtual Rehabilitation 2011, Zurich, Switzerland, June 2011. Full Text PDF
-
G. Burdea, D. Cioi, J. Martin, D. Fensterheim, M. Holenski, The Rutgers Arm II Rehabilitation System - A Feasibility Study, IEEE Transactions on Neural Systems and Rehabilitation Engineering, 18(5):505-514, October 2010. Full Text PDF
-
Supported by:
-
Press Releases.
-
Project Video.
A grant from the Coulter Foundation and by donations to the Tele-Rehabilitation Institute.
Click here to see the press releases.
Participant feedback following Rutgers Arm Feasibility Study. (~35mb MPEG4)
![]() Click here to download the file.
Click here to download the file.
BACK TO TOP